

Providing Better Care for Rare Disease Patients: Primary Care Physician Guide
How can primary care physicians provide the best care for rare disease patients? We’ve researched to compile general information on rare diseases, tips for PCPs on improving care for rare disease patients and families, and educational resources that provide more detailed information on specific diseases and genetic testing.
Access a PDF version of this information at this link.
What is a Rare Disease?
The definition of what “rare disease” means varies by country and/or region.
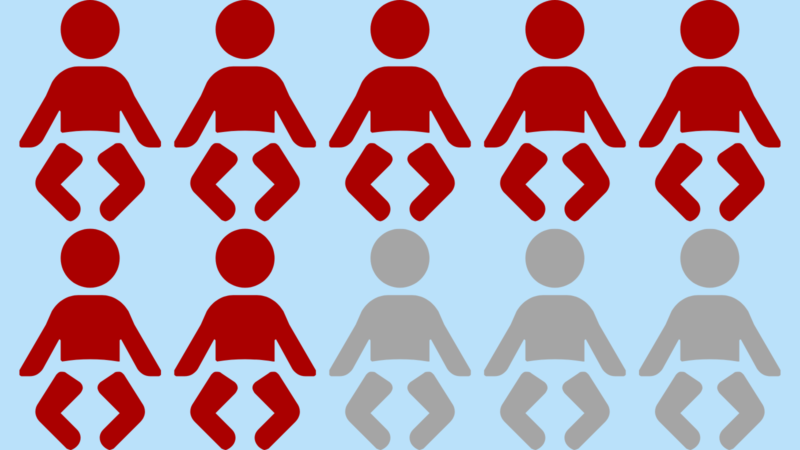
- US: Affects fewer than 200,000 Americans (1)
- Europe: Affects fewer than 1 in 2,000 people (1)
- World Health Organization (WHO): Affects fewer than 65 in 100,000 people (2)

There have been over 7,000 rare diseases identified to date (2)

It’s estimated that rare diseases impact 25-30 million people in the United States (3), and over 300 million people worldwide (2)
Around 70% of rare diseases start in childhood (4)
Genetics are thought to be a factor in many rare diseases (4)
Many rare diseases currently lack effective and/or available treatments
Barriers to Care

Access to care is a significant barrier for rare disease patients. One of the reasons access is an issue is that there is a shortage of medical geneticists, even in high-income countries (5, 6). This insufficient workforce issue is exacerbated by the increased demand for genetic services due to increased awareness and expansion of testing services (7). Both of these things can contribute to long wait times and delays for appointments (8).
Geographical location is another barrier to care (8). Patients may need to travel long distances to see medical geneticists and other specialists. The travel itself may be costly and might require patients or caregivers to take time off work, resulting in lost income (8, 9). Frequent appointments, particularly ones that are far geographically, can also disrupt children’s schooling (8, 9). Some people do not have the ability or means to travel, which may lead to appointments being further delayed or not attended at all (7, 8).

While cost often falls under access to care, we wanted to highlight a few specific issues related to health care costs and insurance separately.
Patients and families with rare disease may face insurance-related barriers, such as being denied coverage for diagnostic testing, specialist visits, or treatments (8, 10). Sometimes insurance will dictate where patients can get specialist care from, and this can further exacerbate travel time and cost concerns. Undiagnosed patients may have an even more difficult time, as a diagnosis can help support medical necessity of a visit, test, or treatment (11). However, even a diagnosis does not prevent all insurance denials.
In the United States, health insurers cannot refuse coverage or charge higher premiums for people because they have a pre-existing condition (12). However, short-term, limited-duration health plans are not required to meet the same quality standards and are sometimes able to discriminate against patients with pre-existing conditions (13). These health plans can also use questionable marketing tactics to lure patients in.
Having health insurance does not guarantee that health care is affordable. A 2025 KFF poll found that 42% of insured US adults found it very or somewhat difficult to afford healthcare costs (14). The poll also found that 36% of respondents said they skipped or postponed care in the last 12 months, and 21% said they have not filled a prescription because of the cost (14).

Poor communication and care coordination between clinicians on the care team can be a barrier to optimal care for rare disease patients. Communication issues are among the most frequent causes of harmful medical errors (15). It’s estimated that about 67% of communication errors relate to handoffs, which is when patient care responsibility transitions from one clinician to another (15).
Poor communication and a lack of care coordination by clinicians can add unnecessary burden and stress for patients and caregivers (17). One study found that patients (or their caregivers) often took on responsibility for coordinating specialty care but struggled to do so (18). When patients and caregivers take on this extra burden, it can cause fatigue, loss of earnings at work, extra travel costs, and extra time off work and school (17).
Information sharing through electronic medical records (EMRs) can contribute to communication challenges. Data in patient charts may be patchwork (emails, faxes, printed docs, EMR notes, etc.) or not available at all, which can make patient care less effective if clinicians do not have all the relevant health information (6).
Many surveys have found that physicians worldwide feel they lack sufficient knowledge about rare diseases and genetic testing (5, 19-21). This lack of knowledge can limit the implementation of recommendations and guidelines (16) and can cause issues with diagnostic delay or misdiagnosis (21). Education on rare diseases and genetic testing can vary by institution and country.
Given the large number of rare diseases, physicians may find it more useful to learn about the specific rare diseases that their patients have. But this isn’t easy. PCPs often don’t have enough time to address all these challenges (5). A 2025 study found that primary care physicians worked an average of 61.8 hours per week (22). Adding in extra work for PCPs without proper tools, resources, or time allotment makes it difficult to put sufficient time into learning about each patient’s rare disease and the latest treatment approaches.

Accurate diagnosis is important to guide treatment, symptom management, and referral to specialists (8). However, many rare disease patients face long delays to diagnosis.
The US Department of Health and Human Services has estimated an average time to diagnosis of five years (8) for rare disease patients. This aligns with findings from a Global Genes study, which reported an average of 4.8 years from symptom onset to correct diagnosis, with some patients experiencing delays up to 20 years (9).
A recent retrospective patient study in Europe found that half of people living with a rare disease waited at least 9 months for a diagnosis after symptom onset, while 25% waited more than 5 years (21). Additionally, a survey conducted in China found a diagnostic delay of an average of 1.4 years for rare disease patients (21).
The diagnostic delay can be taxing, as the typical rare disease patient sees more than seven physicians before getting a diagnosis (9). During this time, patients can experience worsening symptoms or decreased quality of life as they await diagnosis and a more appropriate treatment plan (9).

Guidelines on genetic testing continue to evolve as more information becomes available, but these frequent updates can make it hard for PCPs to stay current on which genetic tests to use and when to use them (7). Even with established guidelines, there are concerns about clarity and feasibility of implementation that may hinder PCPs from scheduling and carrying out recommended tests (16).
Ways Physicians Can Improve Care for Rare Disease Patients
Rare disease patients may see their PCPs more often than other patients. One study found that children with a rare disease (through 14 years of follow-up) had an average of 45.4 primary care visits, while children without had an average of 28.2 visits (23). Primary care clinicians can be a great resource for rare disease patients as they manage their condition. Below are a few ways that primary care physicians can help their rare disease patients and families.
Red Flags
Red flags are clinical features that may suggest a patient has a rare disease. Recognizing these red flags can help primary care physicians pursue appropriate testing and potentially reduce time to diagnosis.
Physician Resources
This section provides links to informational resources for clinicians on rare diseases, including information on diagnosis, management, counseling, genetic testing, and treatment options. Some of these courses offer CME credit, which is denoted within the individual resource blurb below.
Talking to Patients About Clinical Trials
Many rare diseases do not have approved treatments, making clinical trials the best (or only) option for patients. Sometimes patients or caregivers may come to a PCP to ask for guidance about a clinical trial. The following tips may help with navigating these discussions:
Systemic Solutions
Systemic changes would be more impactful to improving rare disease care on a large scale. The following pages outline several approaches that, if implemented broadly, could improve care for rare disease patients and their families.
1. Improve Physician Education
- Provide training and informational resources in genomics and rare disease for physicians in practice (5-7).
- Improve genomics education for physicians in training (19).
- Educate clinicians on interpreting guidelines and making informed decisions about genetic testing. This is important, as guidelines and available tests continue to progress as new research and technologies are discovered (25).
- Within clinics or health systems, consider having short sessions (such as a “Lunch and Learn”) that specialists host to educate PCPs on the latest news in the field and changes to services and treatments offered by those specialists.
2. Provide Clinicians with Appropriate Tools
- Access to whole genome or exome sequencing could reduce the diagnostic odyssey and potentially improve cost-efficiency compared to single-gene tests (9).
- Providing clinical support and decision-making tools can help PCPs provide better care for rare disease patients (5-7).
- AI and machine learning could be used to analyze health records and develop predictive models to expedite diagnosis of rare diseases and improve care (6).
- Ask your administrators if you have access to any tools
3. Set Clear Guidelines and Standards
- Creating clear, evidence-based guidance on genetic testing can help PCPs with frontline testing, and facilitate timely referral of patients and families to appropriate specialists as needed. (5, 6, 25).
- Standardize the approach to getting family history by adopting a universal minimum standard of questions (25). The AMA has a web page called “Collecting a family history” with many good starting points to create these standard questions.
- In the United States, the Recommended Uniform Screening Panel (RUSP) recommends which conditions to test for Newborn Screening, while individual states determine which conditions to include in their screening. As of February 17, 2026, there were 38 core conditions and 26 secondary conditions recommended by RUSP (30). 8 states screen for 64 or more conditions, while 7 states screen for fewer than 38 (31). Standardizing these tests across states may help with better diagnosis (9).
4. Incorporate Genetic Counselors into Primary Care
- Incorporating genetic counselors into primary care clinics could improve patient care (20, 31).
- Genetic counselors could provide primary care support by (31):
- Selecting genetic tests
- Interpreting test results
- Providing pre- and post-test counseling
- Adding genetic counselors to care teams can improve clinical outcomes, increase patient knowledge and engagement, and increase adherence to health plans and healthy behaviors (20, 31).
5. Improve Data Sharing and Communication
- Improve capturing and sharing of patient data, both in the EMR and during in-person communication (6).
- Build more time for communication into the PCP daily schedule.
- Improve ways for patients to view their notes and communicate with PCPs.
6. Telehealth and Appointment Flexibility
- Offer appropriate telehealth options (6).
- Offer appointment flexibility (17).
- Can certain routine or frequent tests be done at PCP office or local clinic instead of a specialist office?
- Can appointments in a similar location be grouped to the same day/times?
- Improve reimbursement for telehealth services.
7. Improve Care Coordination
- Consider adding care coordinators to help patients schedule all necessary appointments in a way that reduces time traveling, time away from work/school, and associated costs.
- Care coordination programs have reported improvements in satisfaction with care, increased interactions with healthcare teams, and reductions in health service use (33).
8. Shorten Time to Diagnosis
- Better genetic testing guidelines may aid PCPs in genetic testing (25).
- Incorporating genetic testing into primary care could streamline testing, reduce time to diagnosis, improve outcomes, and decrease unnecessary specialist visits and travel costs (7, 20, 32).